
Top 9 things you need to know about dysautonomia

Written by Scott Pringle, Founder of the Integrated Health Foundation
- Published on April 15th, 2025
- If you prefer not to read the article or have screen sensitivity, you may listen to this audio version

Table of Contents
- 1. Dysautonomia involves the ANS
- 2. Dysautonomia is a breakdown of the ANS
- 3. There are multiple types of dysautonomia
- 4. Dysautonomia has a wide range of symptoms
- 5. It can be a little tricky to get a dysautonomia diagnosis
- 6. Dysautonomia can be primary or secondary
- 7. Dysautonomia has a rich history
- 8. Long covid has been linked to the rise in dysautonomia cases
- 9. There is hope
Dysautonomia is becoming increasingly common; currently over 70 million people worldwide experience the condition (Cleveland Clinic). Yet, even though dysautonomia is quickly becoming a household name, there is still a lot of confusion and misinformation around what it is, what causes it, and how it presents.
This confusion is especially common because dysautonomia is an “invisible illness” – a type of chronic illness where the people who suffer from it may not appear sick. Due to the number of people afflicted by dysautonomia, it’s likely that you or someone you know has been impacted by it.
This article hopes to answer some of your questions – here are the top 9 things you need to know about dysautonomia.
1. Dysautonomia involves the ANS
Dysautonomia occurs when there is dysfunction of the autonomic nervous system (ANS), so in order to understand what dysautonomia is, we have to first get a concept of the ANS. The autonomic nervous system is a matrix of nerves throughout the body that connect your brain to your organs.
In fact, the ANS is entwined with almost every organ and system in your body. This allows control of your subconscious body functions such as breathing, heart rate, blood pressure, digestion, and many more. These are all processes that run in the background – you don’t have to think about them in order for them to continue; they keep working even when you are asleep (Cleveland Clinic).
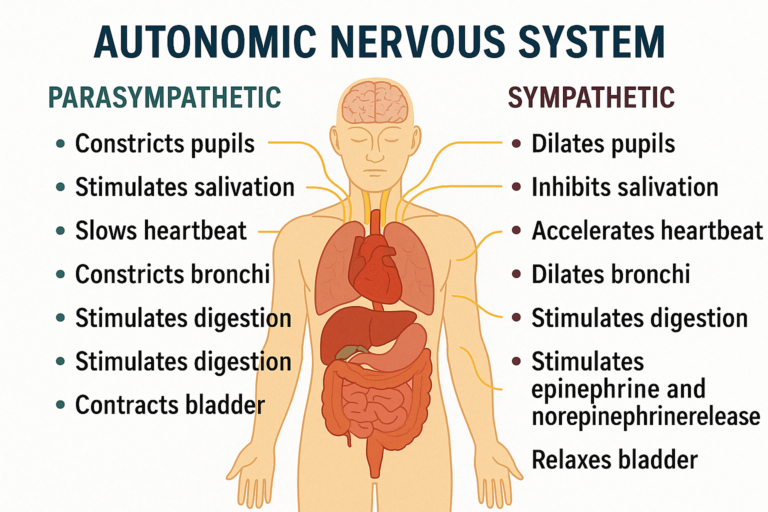
The ANS further divides into two branches known as the sympathetic and parasympathetic nervous systems. These two branches work oppositely of each other to maintain balance in the body.
You can think of the sympathetic nervous system like the “gas pedal” of your body; it revs things up and allows you to escape from danger (the fight or flight response). On the flip side, you have the parasympathetic nervous system which works like your body’s “brake pedal”; it calms things down (the rest and digest functions).
In a healthy, functioning body, these two systems work together to keep all of your organ systems running smoothly (Cleveland Clinic).
So what happens when this system isn’t balanced and working the way it’s supposed to? Enter: dysautonomia.
2. Dysautonomia is a breakdown of the ANS
Let’s keep going with our car analogy. Imagine driving somewhere, and as you’re driving you alternate between using your gas and brake pedals. This allows you to maintain a safe driving speed, stop at appropriate places, or accelerate quickly to get out of the way of potential mishap.
How well do you think you could drive if your brake lines were cut, and it was impossible for you to stop when you needed to? Or if, in addition to no brakes, there was a brick on your gas pedal hurtling you at breakneck speeds down the road, and you could only attempt control with wild steering? What if you were trying to drive with both your gas and brake pedals completely floored at the same time?
Just as these would not be safe or functional ways to drive, when our body’s “gas and brake pedals” (the sympathetic and parasympathetic nervous systems) are not functioning the way they are supposed to, it can wreak havoc.
Dysautonomia, then, is the name for any condition that disrupts the autonomic nervous system. It can range in severity from extremely mild to debilitating, and can affect a variety of organs. Dysautonomia is sometimes also referred to as autonomic dysfunction or autonomic neuropathy (Cleveland Clinic).
Since dysautonomia is a condition of the nervous system which primarily affects internal organs, this is what contributes to it being considered an “invisible illness”. However, this doesn’t mean that those who have this condition are faking or playing up their symptoms and struggles!
Even though outward signs of the condition are less common, the impact on quality of life can be enormous. Just as with any other illness, those with dysautonomia need compassion and support, even if you don’t see physical manifestations of their condition.
3. There are multiple types of dysautonomia
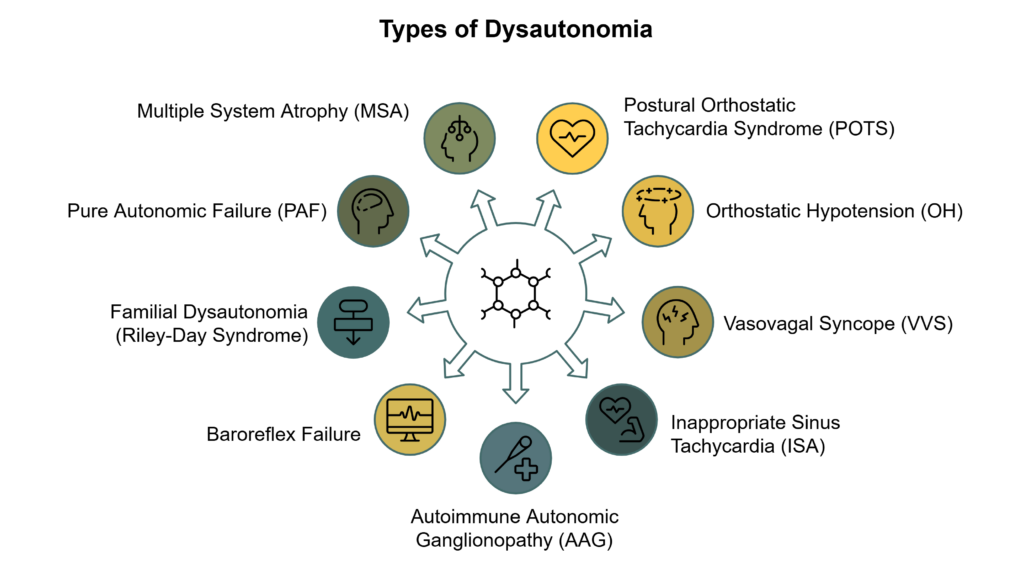
Dysautonomia is an umbrella term for many conditions of the autonomic nervous system. It involves a broad spectrum of symptoms and severities, which can significantly impact daily living. It is also possible to experience and be diagnosed with more than one type of dysautonomia at a time. A few of these conditions include the following:
- Postural Orthostatic Tachycardia Syndrome (POTS) – Characterized by an excessive heart rate increase upon standing among other symptoms. This is the most common form of dysautonomia, with an estimated 500,000-3 million Americans having the condition.
- Orthostatic Hypotension (OH) – A form of low blood pressure that happens when standing up from sitting or lying down.
- Vasovagal Syncope (VVS) – Also known as neurally mediated syncope (NMS), this is a common form of fainting that occurs in response to a trigger, such as prolonged standing or emotional stress.
- Inappropriate Sinus Tachycardia (ISA) – A chronic condition where the heart rate is over 100 beats per minute while at rest.
- Autoimmune Autonomic Ganglionopathy (AAG) – Also known as acute pandysautonomia, characterized by orthostatic hypotension, numbness in the hands and feet, among other symptoms.
- Baroreflex Failure – Happens when there is a failure of the baroreflex mechanism, which helps maintain a stable blood pressure.
- Familial Dysautonomia (Riley-Day Syndrome) – A rare genetic disorder that affects the sensory and autonomic nervous systems.
- Pure Autonomic Failure (PAF) – A degenerative disease of the autonomic nervous system that causes severe orthostatic hypotension.
- Multiple System Atrophy (MSA) – A progressive neurodegenerative disorder characterized by autonomic dysfunction and motor impairment.(Dysautonomia Support)
4. Dysautonomia has a wide range of symptoms

Think again about all of the body systems that the ANS is involved in (essentially all of them). Because of this, dysautonomia can look different based on which organs are involved.
The primary symptoms that most people experience are:
- Fatigue
- Dizziness
- Brain fog
- Shortness of breath
- Difficulty sleeping
- Poor circulation and blood pooling in feet and legs
However this can vary from person to person. If your eyes are affected by your nervous system dysfunction, you may experience vision changes, blurriness, wide or pinpoint pupils, and dry or watery eyes.
If your cardiovascular system is being affected, you may have tachycardia, blood pressure changes, or blood pooling in your legs and feet.
The symptoms of dysautonomia can seem extremely varied and disconnected, which is why seeing a practitioner who understands dysautonomia is very important (Cleveland Clinic).
5. It can be a little tricky to get a dysautonomia diagnosis

What do headaches, poor digestion, and heart palpitations have in common? This seeming disconnection between symptoms can be one of the struggles when trying to get dysautonomia diagnosed. Many physicians hyper-specialize in their own areas – neurology, gastroenterology, cardiology, and so on.
But, of course, all of those symptoms and systems are connected to the ANS. Unfortunately, when a condition such as dysautonomia is present, there’s not just a single system or organ involved; a full body picture is necessary to truly understand what’s going on.
Because of this, finding a physician who is familiar with (or even specializes in) dysautonomia is essential to receiving prompt and adequate care. The types of physicians who treat dysautonomia range across many specialties, but the most common are neuromuscular doctors, cardiologists, and neurologists. Organizations such as The Dysautonomia Project have physician finder links to assist individuals in finding a provider near them.
Once an appropriate physician has been located, they are able to walk clients through the specific tests that can be helpful in obtaining a diagnosis. Often, dysautonomia is a diagnosis of exclusion, and it can take quite a bit of time and teamwork to obtain an official diagnosis (Cleveland Clinic).
6. Dysautonomia can be primary or secondary
“Primary” dysautonomia means that it happens on its own, without a specific cause. One of these is familial dysautonomia – an inherited genetic condition. Certain demographics are at higher risk for familial dysautonomia, and that may be taken into consideration when seeking a diagnosis. “Idiopathic” dysautonomia is also considered a primary form of the condition; medical professionals don’t know what caused it, so it’s placed in this category (Cleveland Clinic).
Far more commonly, dysautonomia is “secondary”, meaning it has a specific condition that caused or contributed to it. There are many of these conditions, some of which include:
- COVID-19
- Lyme
- EDS and other connective tissue disorders
- MS
- Toxins such as mold or heavy metals
- Lupus
- Traumatic brain injury
- And many more (Cleveland Clinic)
Many people with dysautonomia are able to link the beginning of their illness to a “trigger” event (or, more often, a “perfect storm” of events). As the cause can be extremely varied, it can be helpful to determine what the root cause of the condition was and when the trigger event occurred. Despite the diversity of causes, however, the approach to managing dysautonomia tends to follow a unified path focusing on re-regulating the nervous system.
7. Dysautonomia has a rich history
We often think of conditions such as dysautonomia as new problems, unique to our modern society. However, even though there wasn’t a name for it yet, many historical cases describe what we now believe to have been dysautonomia. Even the accounts of King David in the 10th century BC seem to be consistent with symptoms that can be caused by dysautonomia – primarily difficulty with his balance and temperature regulation (Very Well Health).
In the late 19th century, the dysautonomic condition “beriberi” (translated to “I can’t, I can’t”) became prevalent among the Japanese navy, causing a high number of deaths. Japanese naval doctor Kanehiro Takaki made major breakthroughs with his research, finding that officers who ate a varied diet with more protein were less likely to develop the condition than the soldiers who ate primarily white rice. By altering the sailors’ diets, he was able to drastically reduce the number and severity of beriberi cases on the voyage.
His study was one of the first to indicate that beriberi was not an infectious disease, as previously thought, but rather a nutritional deficiency. His research laid the groundwork for later progress, including the discovery of vitamins. (The James Lind Library).
What we now understand about Takaki’s findings is that a diet low in meat and high in white rice causes thiamine (B1) deficiency. This vitamin deficiency, in turn, is responsible for the symptoms of beriberi. The role of thiamine deficiency in dysautonomia has been well-documented, and the reversal of this deficiency can be key in treating the condition (Lonsdale, 2006).
8. Long covid has been linked to the rise in dysautonomia cases
Since the beginning of the COVID-19 pandemic, a demographic of people who experience long COVID has emerged. According to CDC numbers from 2022, 7.5% of US adults experienced long covid symptoms. In order to be considered long COVID, these symptoms lasted three months or longer from the time of initial infection, and were not present before the illness happened (CDC).
In early 2022 the journal Frontiers in Neurology published a study evaluating the link between long COVID and dysautonomia. What they discovered is that, of the 2,314 global long COVID sufferers they surveyed, 67% were found to have moderate to severe autonomic dysfunction. As mentioned in the beginning of this post, there are now 70 million people worldwide afflicted with dysautonomia, many of whom experienced COVID-19 as their trigger event (News Medical).
9. There is hope

Everything you’ve learned about dysautonomia up until this point may seem incredibly daunting. In truth, the modern western medical belief is that dysautonomia is an incurable, lifelong chronic illness. For some, it’s no more than a slight annoyance; for others, it can be a debilitating condition that leads to becoming bedridden.
If you or someone you love is affected by dysautonomia it can be frustrating, isolating, even terrifying. However, thanks to the internet, online support groups and communities are popping up, allowing people to connect with others who truly understand what they are going through.
Furthermore, many who find themselves experiencing the trials of dysautonomia are turning to more holistic approaches to manage their symptoms and improve their overall health. There are many who have successfully put their dysautonomia into remission for years through dietary, lifestyle, and nervous system regulation practices.
We have found that education, support, and holistic care are the cornerstones of helping people manage their dysautonomia symptoms.
Evaluate Your Symptoms: Do You Have Dysautonomia?
Take our quick and comprehensive symptom assessment to find out if your symptoms align with dysautonomia and receive personalized insights.
Share This Article
Read More Articles

Is Your Nervous System Overmedicated or Under supported?
Calm your overactive nervous system naturally: root causes, real healing tools & steps to feel safe again. Take our free assessment today!

What is a Dysregulated Nervous System?
Discover what a dysregulated nervous system is, explore symptoms & recovery options, and take our free Symptoms Assessment today!

What is the Carnivore Diet: Benefits, Risks, and Science Explained
Explore the Carnivore Diet: benefits, risks & real results for chronic illness. Take our free health assessment today!
